In 2020, Jerry Fontana of Scranton, Pennsylvania, received horrible news: Doctors in Scranton diagnosed him with late-stage liver cancer.
“I was very, very sick. I couldn’t eat, I couldn’t sleep. I was in total pain all the time,” Fontana said. “They told me to get my life in order. I have maybe 3 to 6 months to live.”
That was four years ago.
Fontana went to Johns Hopkins’ in Baltimore and participated in an early-stage clinical trial led by Dr. Mark Yarchoan.
Researchers developed and tested a personalized vaccine aimed at shrinking tumors, used in combination with a type of immunotherapy for hepatocellular carcinoma, which is the most common form of liver cancer.
“This is a cancer that normally, in most cases arises out of a sick liver. So patients with cirrhosis from any cause such as hepatitis B, hepatitis C. Increasingly you see particularly in the United States, patients with alcohol or fatty liver disease,” said Yarchoan.
Fontana, along with 35 others were given an immunotherapy drug alongside the vaccine. Liver cancer is one of the leading causes of cancer deaths worldwide, accounting for over 700,000 deaths each year, according to the American Cancer Society. Liver cancer rates have more than tripled since 1980; the death rates have more than doubled during this time.
Now, researchers have developed a personalized vaccine to fight tumors in liver cancer patients and are running it in clinical trials. Vaccines work by super-charging our immune systems, so while we may think of them only for prevention of illnesses like the flu or COVID, they’re used in treatment too. The personalized anti-tumor vaccines are made of specific DNA to target mutated cancer genes. The DNA is derived from a patient’s own biopsy of their tumor. Roughly a third of the patients’ tumors shrunk.
“Patients had continued tumor control for, in many cases, months or years,” said Yarchoan.
Fontana’s tumor did not shrink much — so he’s not counted in that 30%. But the cancer levels in his blood dropped, Yarchoan explains.
“We may be underestimating the total number of patients who benefited from the treatment when we give that sort of top-line number of around 30% of patients having tumor shrinkage, because clearly there are patients who’ve benefited beyond that number,” he said.
Fontana is now in a second trial for liver cancer patients at Johns Hopkins, and with a second lease on life — one he refuses to squander. He’s active, and tells Scripps News he’s happy to participate in medical research to pay it forward. He’s back to work too.
“I’m fixing cars and I actually work. So I’m working three days a week, four hours a day. You know, just keep busy because I’m retired, you know? I got to live life. That’s tough to do when I want to go fishing,” said Fontana, with a smile.
Researchers from Singapore and the UK used mouse models, human tissue, and human breast organoids grown in the lab to find that changes in glucose metabolism could help cancer grow by temporarily disabling a gene that protects us from tumors called BRCA2.
“These findings raise awareness of the impact of diet and weight control in the management of cancer risks,” says the first author of the new study, cancer pharmacologist Li Ren Kong from the Cancer Science Institute of Singapore (CSI Singapore).
“We started the study aiming to understand what factors elevate risk in families susceptible to cancer, but ended up discovering a deeper mechanism linking an essential energy consumption pathway to cancer development.”
The discovery also challenges a long-established theory about genes that protect against cancer. Knudson’s ‘two-hit’ paradigm, first proposed in 1971, states that both copies of a tumor suppressor gene must be permanently inactivated in our cells before cancer can start.
In mice, having just one copy of BRCA2 affected doesn’t seem to cause major issues in organ development or DNA repair in most tissues. But cells with this mutation appear more vulnerable to stresses, like exposure to environmental toxins such as formaldehyde or acetaldehyde, which can reduce their levels of BRCA2 protein, leading to functional problems.
“How such environmental factors increase cancer risk is not yet very clear, but it is vital to understand the connection if we are to take preventive measures that help us stay healthy longer,” says oncologist and cancer researcher Ashok Venkitaraman from CSI Singapore.
The team first examined people who inherited one faulty copy of BRCA2. They found that cells from these people were more sensitive to methylglyoxal (MGO), which is produced when cells break down glucose for energy in the process of glycolysis.
Glycolysis generates over 90 percent of the MGO in cells, which a pair of enzymes typically keep to minimal levels. In the event they can’t keep up, high MGO levels can lead to the formation of harmful compounds that damage DNA and proteins. In conditions like diabetes, where MGO levels are elevated due to high blood sugar, these harmful compounds contribute to disease complications.
The researchers discovered that MGO can temporarily disable the tumor-suppressing functions of the BRCA2 protein, resulting in mutations linked to cancer development. This effect could be seen in noncancerous cells as well as patient-derived tissue samples, in some cases of human breast cancer, and in mouse models of pancreatic cancer.
As the BRCA2 allele isn’t permanently inactivated, functional forms of the protein it produces can later return to normal levels. But cells repeatedly exposed to MGO may continue to accumulate cancer-causing mutations whenever existing BRCA2 protein production fails.
Overall, this suggests that changes in glucose metabolism can disrupt BRCA2 function via MGO, contributing to the development and progression of cancer.
These results come from lab tests and small human tissue sample sizes, and the researchers say more studies need to be done using larger clinical studies or animal models to look into possible links between dietary factors, diabetes, and other metabolic disorders.
As MGO can temporarily rob the BRCA2 protein of its ability to repair DNA, it makes sense that a poor diet or uncontrolled diabetes could contribute to a higher risk of cancer over time, even in people with two functional copies of the BRCA2 gene. This new information may lead to strategies for cancer prevention or early detection.
“Methylglyoxal can be easily detected by a blood test for HbA1C, which could potentially be used as a marker,” Venkitaraman says.
“Furthermore, high methylglyoxal levels can usually be controlled with medicines and a good diet, creating avenues for proactive measures against the initiation of cancer.”
Where will the annular solar eclipse on Oct. 2, 2024 be visible? – Space.com
An annular solar eclipse will occur on Oct. 2, 2024, when the moon’s central shadow will not quite reach Earth. The result will be a ‘ring of fire’ visible to those within a broad path across the Pacific Ocean and southern South America.
At the point of greatest eclipse in the Pacific, the moon will cover 93% of the sun’s center, and that ‘ring of fire’ will be visible for 7 minutes and 25 seconds.
This annular solar eclipse has a long and broad path, rising south of Hawaii in the North Pacific Ocean and setting north of South Georgia in the South Atlantic Ocean. That journey is a mighty 8,800 miles (14,163 kilometers), with the path between 165 and 206 miles (265 to 331 km) wide. Very little of it crosses land, with only Rapa Nui (Easter Island) and southern parts of Chile and Argentina in South America within the path of annularity.
The global path of the ‘ring of fire’ annular solar eclipse on Oct. 2, 2024. (Image credit: Created and annotated by Jamie Carter using MapHub.net. Source: Esri, Maxar, GeoEye, Earthstar Geographics, CNES/Airbus DS, USDA, USGS, AeroGRID, IGN, and the GIS User Community)
The path of annularity: Rapa Nui (Easter Island)
Rapa Nui (Easter Island) is entirely within the path of the annular solar eclipse on Oct. 2, 2024. (Image credit: Created and annotated by Jamie Carter using MapHub.net. Source: Esri, Maxar, GeoEye, Earthstar Geographics, CNES/Airbus DS, USDA, USGS, AeroGRID, IGN, and the GIS User Community)
It’s a marvel that the ‘ring of fire’ will be visible from this remote volcanic island in the South Pacific, halfway between Tahiti and South America. It’s been only 14 years since a total solar eclipse was visible from here on July 11, 2010.
About 2,200 miles (3,540 km) west of Chile, Rapa Nui is home to 1,000 mysterious moai, the remnants of a culture from the 13th–16th centuries. Perched on stone pedestals called ahus, these carved human figures can be found at several sites on the island, which is entirely within the eclipse’s path.
Breaking space news, the latest updates on rocket launches, skywatching events and more!
The ‘ring of fire’ will hang 67 degrees above north and last 6 minutes 28 seconds at Rapa Nui’s most southerly point, Orongo, and 5 minutes 59 seconds at its most northerly point, Ana o Heu.
The path of the ‘ring of fire’ annular solar eclipse through South America on Oct. 2, 2024. (Image credit: Created and annotated by Jamie Carter using MapHub.net. Source: Esri, Maxar, GeoEye, Earthstar Geographics, CNES/Airbus DS, USDA, USGS, AeroGRID, IGN, and the GIS User Community)
Barely 1,000 miles (1,600 km) of the 8,800 miles (14,163 km) path of annularity crosses land on Oct. 2, 2024, the vast majority of it in southern South America and two countries in particular — Chile and Argentina. Chile’s Pacific Coast is difficult to access, but Carretera Austral (also called Route 7) dissects the path in rural Patagonia’s Aisén region. As it strikes Chile, the eclipse will be 26 degrees above the north-northwest horizon, with the lower elevation arguably creating a more dramatic sight than from Rapa Nui (Easter Island).
Key locations in Chile include Cochrane, close to the centerline (south along the Carretera Austral), and Chile Chico, just outside the northern limit, close to the border with Argentina. The latter would be a good choice for anyone wanting to see extended displays of Baily’s beads, which could last a few minutes.
In Argentina, a choice location in a wild, empty region could be Perito Moreno National Park. For a more arid eclipse with the highest chances of a clear sky anywhere in the path, choose Puerto Deseado and Puerto San Julián in Santa Cruz Province on Argentinean Patagonia’s Atlantic coast.
The next annular solar eclipse: 2024 vs 2027
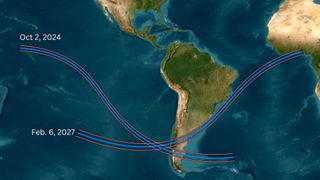
The paths of annularity on Oct.2, 2024, and Feb. 6, 2027 (left) and where they cross (right). (Image credit: Created and annotated by Jamie Carter using MapHub.net. Source: Esri, Maxar, GeoEye, Earthstar Geographics, CNES/Airbus DS, USDA, USGS, AeroGRID, IGN, and the GIS User Community)
On average, a central solar eclipse occurs in the same place twice every 366 years or so, according to NASA, but two-and-a-half years after 2024’s annular solar eclipse, another happens partly in the same place. On Feb. 6, 2027, a 7-minute and 51-second ‘ring of fire’ will again be visible again from Chile and Argentina.
The 2024 and 2027 paths cross just off the coast of Chile in the Pacific Ocean. In 2027, the path will cross Chile slightly to the north of the 2024 path, while in Argentina, it swerves through central Patagonia and misses the capital city, Buenos Aires. It also just missees Montevideo, the capital of Uruguay, shaving that country’s southeast coast before traveling across the Atlantic to show a ‘ring of fire’ sunset to those in Côte d’Ivoire, Ghana, Togo, Benin and Nigeria.
Additional resources
Want to look further ahead? You can find a concise summary of solar eclipses out to 2030 on NASA’s eclipse website. Read more about solar and lunar eclipses on EclipseWise.com, a website dedicated to predictions of eclipses. See beautiful maps on eclipse cartographer Michael Zeiler’s GreatAmericanEclipse.com and interactive Google Maps on Xavier Jubier’s eclipse website. You can find climate and weather predictions by meteorologist Jay Anderson on eclipsophile.com.
Bibliography
Anderson, J. (February 2024). Annular Solar Eclipse
Nepal on alert for more snakebite cases as summer approaches – South China Morning Post
While Kharel received timely treatment, many others in Nepal are less fortunate. Snakebites remain a pervasive and deadly threat in the country, especially among its rural populations, but experts believe that targeted awareness campaigns and increased treatment access could halve the number of fatalities.
Nepal’s Toxinology Association hosts a snakebite awareness programme at a school. Globally, nearly 138,000 people die of snakebites annually, according to the WHO. Photo: Kamal Devkota
A 2022 research in the medical journal The Lancet, which is said to be the first snakebite epidemiological study in Nepal, estimated that there were as many as 37,661 snakebite cases and 3,225 deaths annually in the country’s southern plains. However, the government’s hospital-reported data from the past two decades show an average of 20,000 hospitalisations and about 1,000 deaths every year.
Globally, nearly 138,000 people die of snakebites annually, according to data from the World Health Organization, with one 2019 study estimating that 70 per cent of those casualties are in South Asia.
In 2017, the WHO listed snakebites as a neglected tropical disease due to a lack of attention it receives from the global health agenda.
In countries like Nepal, doctors say a reliance on traditional healers and unproven techniques, as well as delays in receiving critical medical interventions during the first few hours after being bitten, often lead to deaths.
“Around 80 per cent of people die before reaching hospitals,” Sanjib Kumar Sharma, a professor at the BP Koirala Institute of Health Sciences in eastern Nepal, told This Week in Asia. “The cause of death is often due to delay in transport.”
04:35
Myanmar’s ‘Snake Princess’ hopes to wrangle and dispel reptile fears one snake at a time
Myanmar’s ‘Snake Princess’ hopes to wrangle and dispel reptile fears one snake at a time
‘Neglected disease’
The districts in Nepal’s southern lowlands are the most vulnerable to snakebites due to the warmer climate and reptile habitats throughout the region. There are some 89 species of snakes in Nepal, though most common bites come from the cobra, krait and viper families.
Research and anecdotal evidence from doctors show that snakebites disproportionately affect women and children in Nepal’s remote villages, both indoors and outdoors.
Many girls and women have succumbed to snakebites while staying in outdoor spaces during menstruation due to archaic Hindu traditions that banishes them during their monthly cycle.
Krishna Acharya, an anaesthesiologist who worked in the government-run Bheri Hospital in Nepalgunj, treated over 2,000 snakebite patients during his eight-year tenure that ended this year.
He was initially untrained to handle snakebite patients but received training after seeing an influx of patients who had their care delayed after having to be referred to a designated snakebite treatment centre.
It’s a neglected disease because it affects the poor, and those in the city, expect a few exceptions, aren’t affected by snakebites. That’s why there’s little interest in it
Krishna Acharya, National Trauma Centre
There are more than 110 snakebite treatment centres nationwide, mostly in public hospitals or treatment centres that are run by the Nepali army and Nepal Red Cross. The government has also published national guidelines for snakebite management – detailing clinical manifestations, diagnosis and management of snakebite envenoming – and provides free antivenom vials.
But doctors say that is not enough, as the country lacks trained medical professionals to manage snakebites and treatments can be expensive.
Snakebite treatment costs about 10,000 rupees (US$75) on average and can go as high as 400,000 rupees if patients require intensive care and life support, an astronomical amount for many living in Nepal’s villages, according to Acharya.
Acharya, who now works at Kathmandu’s National Trauma Centre, said the country’s medical colleges rarely teach about snakebites, resulting in doctors being unable to handle such cases. Sharma recommended that chapters on locally found snakes and treatment techniques be included in the curriculum.
“Many people who shouldn’t die of snakebites are dying in Nepal,” Acharya said. “It’s a neglected disease because it affects the poor. Those in the city, except for a few exceptions, aren’t affected by snakebites. That’s why there’s little interest in it.”
A Nepalese boy seeks blessings after worshipping the snake god “Nag” at the Nagpokhari Kathmandu temple. Snakebites disproportionately affect women and children in Nepal’s remote villages, both indoors and outdoors. Photo: Reuters
Not all snakes are venomous
Kamal Devkota, a conservation biologist, has been studying snakes for years and works at the Nepal Toxinology Association to research and educate people on snakebites and snake conservation.
Though snakes are worshipped in Hinduism, a predominant religion in Nepal, he said people largely kill snakes out of fear and a lack of information about poisonous species.
Devkota said that habitat loss due to infrastructure development and wildfire in summer months have pushed many snake species into human settlements, mostly in search of food. Human-snake conflict has led to not just an increased number of snakebites but also the killing of snakes, which has an impact on the ecosystem.
“Snakes are said to be farmers’ friends,” Devkota told This Week in Asia. “They help in pest control in farms, which would help increase productivity and also minimise the use of pesticides. If their population decreases, then it also impacts other birds of prey that depend on snakes.”
A devotee holds a snake to show his devotion and respect, and to seek blessings during the snake festival in Kathmandu. Snakes are worshipped in Hinduism, a predominant religion in Nepal. Photo: Reuters
Doctors and conservationists say the reptiles are also important medically, especially in Nepal, for research into life-saving antivenoms for lesser known and newly found poisonous snakes. Currently, Nepal imports antivenoms from India which are mostly made for “the big four” available there – the Indian cobra, common krait, Russell’s viper and the saw-scaled viper.
Limited antivenom imports mean there is often short supply in treatment centres and doctors say their effectiveness for certain species is lower and carries higher chances of causing adverse reactions in patients.
“We need regional antivenom specific to local snakes,” said Sharma, also the co-author of The Lancet study.
But so far, Nepal does not have plans to invest in producing its own antivenoms and efforts by private companies have not materialised yet.
“How much of the antivenom produced in Nepal will be put into use?” asked Hemant Chandra Ojha, chief of the zoonotic and communicable disease control section in Nepal’s Epidemiology and Disease Control Division. “The demand is very low, so it wouldn’t be sustainable.”
05:12
Snakes on a plate: world’s first snake soup pizza put to the taste test
Snakes on a plate: world’s first snake soup pizza put to the taste test
Push for awareness
Experts say one of the major ways to save lives from snakebites is through public awareness campaigns at the community level. Another is expanding snakebite treatment centres offering antivenoms in remote areas.
The Epidemiology and Disease Control Division, along with the Rotary Club of Kathmandu Mid-Town, have initiated campaigns to disseminate information on preventive measures using local languages spoken in the southern region. They include messages to households about keeping their surroundings clean, sleeping under a net, and being aware of walking at night, when there is greater chances of snakebites.
However, Acharya believes that awareness campaigns highlighting preventive measures are not enough to save lives.
“People need to have information on where the snakebite treatment centres are and they should be easily accessible to them for timely care,” he said. “If we have targeted campaigns and focus on snakebite affected areas, the mortality can be halved.”
Green bamboo snake. Experts say one of the major ways to save lives from snakebites is through public awareness campaigns at the community level. Photo: Shutterstock
Meanwhile, there are also initiatives to train more healthcare providers, including paramedics, who doctors say play a crucial role in saving people from snakebites.
Ojha said that the government is educating medical students at its National Academy of Medical Sciences, who are deployed to various government hospitals after graduating, as well as scaling up services in at-risk areas and adding new human resources annually through training.
At the community level, snakebite survivors like Khanal are also helping raise awareness. She said those in her neighbourhood have become more conscientious after last year’s incident.
“I mostly share what I experienced,” she said. “I tell them that you need to go to the hospital as soon as possible. They saw how it helped me survive, so people around me are more aware now.”