Entertainment news
Ancient, 30-foot ancestor of great white shark unearthed in Mexico quarry – Livescience.com

Complete fossils from an enormous shark that lived alongside the dinosaurs reveal crucial information about this enigmatic predator — including it being an ancient relative of the great white shark.
The sharks, from the genus Ptychodus, were first discovered in the mid-eighteenth century. Descriptions of this genus were largely based on their teeth — which could be nearly 22 inches (55 centimeters) long and 18 inches (45 cm) wide, and were adapted for crushing shells — found in numerous marine deposits dating to the Cretaceous period (145 million to 66 million years ago).
Without the ability to examine a fully intact specimen, researchers had hotly debated what the shark’s body shape might look like — until now.
“The discovery of complete Ptychodus specimens is really exciting because it solves one of the most striking enigmas in vertebrate paleontology,” lead author Romain Vullo, a researcher at Géosciences Rennes, told Live Science in an email.
In a study published Wednesday (April 24) in the journal Proceedings of the Royal Society B: Biological Sciences, researchers have described complete fossils of the shark discovered in limestone quarries in Nuevo León, northeastern Mexico. Its outline was still fully preserved, and its body shape suggests it hunted sea turtles — which could explain its extinction around 76 million years ago as it was competing with other animals that ate the same prey.
The specimens “show an exquisite preservation,” because they were deposited in a quiet area with no scavengers, Vullo said. “The carcasses of animals were rapidly buried in a soft lime mud before being entirely disarticulated.”
Analysis of the fossils reveals this large predator belonged to the mackerel shark group (Lamniformes), which includes great whites (Carcharodon carcharias), mako, and salmon sharks. It grew to around 33 feet (10 meters) long and is known for its massive, grinding teeth, which are unlike those we see in sharks today.

It was widely believed that Ptychodus fed on invertebrates from the seabed — the ancient relatives of clams and mussels. But the new fossils challenge that, revealing that this ancient shark had a streamlined body shape, indicating it was a fast-swimming pelagic predator. “The newly discovered fossils from Mexico indicate that Ptychodus looked like the living porbeagle shark,” Vullo said, but with “unique grinding dentition.”
This new information has led the researchers to believe it preyed on large ammonites — a type of crustacean with a hard shell — and sea turtles.
“Ptychodus occupied a special ecological niche in Late Cretaceous seas,” Vullo said, because it was the only pelagic shark that was adapted to eating hard-shelled prey such as turtles. This may explain why it died out around 10 million years before the extinction event that ended the Cretaceous period. “Toward the end of the Cretaceous, these large sharks were likely in direct competition with some marine reptiles (mosasaurs) targeting the same prey,” he said.
Entertainment news
Dry eye and some related factors in patients with T2DN | OPTH – Dove Medical Press

Introduction
Dry eye is a multifactorial disease of the tears and ocular surface that results in symptoms of discomfort, visual disturbance, and tear film instability with potential damage to the ocular surface. It is accompanied by increased osmolarity of the tear film and inflammation of the ocular surface.1 Dry eye is a relatively common condition with a global prevalence ranging from 20% to 50%, depending on the evaluation criteria with symptoms, signs alone or in combination.2 Dry eyes negatively affect vision and quality of life.3–5
Diabetes mellitus is one of the most common metabolic diseases in the world. As of 2021, there will be 537 million people with diabetes worldwide. This number is expected to increase to 643 million people in 2030 and 783 million people in 2045.6 Kidney complications and eye complications are common in diabetic patients. Eye complications, including dry eyes, are an early complication in patients with type 2 diabetes mellitus (T2DM). The prevalence of dry eyes in T2DM patients also ranges from 15% to 53%.7–10 The pathogenesis of dry eye caused by type 2 diabetes is mainly related to peripheral corneal neuropathy, tear film instability, ocular surface inflammation, and the apoptosis of conjunctival epithelial cells.11 Another mechanism involved is that with prolonged hyperglycemia, tear osmolarity increases, while conjunctival mucus secretion is significantly reduced, leading to decreased tear secretion and increased tear film instability.12,13
In fact, kidney complications and eye complications often go together, and “renal-retinal syndrome” originates from this coincidence.14 There have been many studies on dry eyes in diabetic patients. However, the prevalence of dry eyes and related factors in patients with type 2 diabetic nephropathy has not been studied much. We conducted this study to investigate the association between dry eye and renal complications in T2DM patients.
Patients and Methods
Patients
A total of 245 patients diagnosed with type 2 diabetic nephropathy (T2DN) were monitored and treated at Nghe An Friendship General Hospital, Nghe An province, Vietnam, from January 2022 to January 2023. Patients were diagnosed with diabetic nephropathy (DN) as had one in 3 following criteria: positive microalbuminuria; macroalbuminuria; estimated glomerular filtration rate (eGFR) < 60 mL/min/1.73m2 equal or more than 3 months. We excluded patients with ophthalmological inflammatory complications, contact lens users, prior eye surgery, or those taking medications associated with dryness. Patients on hemodialysis; acute infection; suspected surgical disease; pregnant or lactating women were also excluded from this study. The remaining 169 patients who met the criteria wrote a written informed consent to participate in this study voluntarily. We also used 169 patients diagnosed with type 2 diabetic mellitus (T2DM), without renal complications, as the control group to participate in this study. We collected all data on clinical characteristics and laboratory parameters at the baseline time of the study.
The Ocular Surface Disease Index (OSDI) and fluorescein tear-film break-up time (TBUT) were done on a total of 338 patients according to standard recommendations.15,16 The above two indexes were performed by ophthalmologists at the Nghe An Eye Hospital. OSDI is a 12-item questionnaire that scores the dryness symptoms on a scale from 0 to 100. Patients with values of 0–12 are considered normal, from 13 to 22 with light, from 23 to 32 with moderate, and values >32 (33–100) with severe symptoms.15 TBUT was measured for each eye 3 times, and the TBUT value of the measured eye was the average of the 3 measurements. Fluorescein staining and TBUT measurements will be repeated in the remaining eye. For statistical purposes, the TBUT value was the worst result from both eyes. Patients with TBUT values equal to or under 10 seconds in at least one eye are determined to have dry eye.16
Disease duration, blood pressure, peripheral nerve complications, treatment data, hematological and biochemical indexes such as urea, creatinine, albumin, protein, high sensitive C-reactive protein (CRP-hs) as well as fasting glycemia and HbA1c were collected simultaneously with the Schirmer test. Lipid disorder was confirmed by testing lipid parameters when there was one or more disorders such as blood cholesterol > 5.2 mmol/L (200 mg/dL); triglycerides > 1.7 mmol/L (150 mg/dL); LDL-cholesterol > 2.58 mmol/L (100 mg/dL) and/or HDL-cholesterol < 1.03 mmol/L (40 mg/dL).
Statistical Analyses
All the normal distribution continuous data were represented by mean and standard deviation and were analyzed using the Student’s t-test. The skewed distributions were described by median (25 percentile – 75 percentile) and analyzed using the Mann Whitney U and Kruskal Wallis tests. Categorical data were presented by the frequency and were analyzed using the Chi-square test. Multivariable adjusted regression analysis was performed to identify the independent factors related to dry eye. Statistical analysis was performed using Statistical Package for Social Science (SPSS) version 20.0 (Chicago, IL, USA) with a p-value <0.05 was considered significant.
Results
Table 1 shows the T2DN group had mean age, the median duration of DM, the proportion of hypertension, peripheral nerve complications, anemia, lipid disorder, plasma urea, creatinine, CRP-hs, the proportion of using insulin higher than those of T2DM, p< 0.01, 0.001. The T2DN group’s OSDI score was higher, but the TBUT was significantly lower than the T2DM group, p<0.001. The prevalence of dry eyes in the T2DN group was significantly higher than in the T2DM group, p < 0.001.
 |
Table 1 Comparison of Demographic and Laboratory Characteristics in Group 1 and Group 2 |
The results in Table 2 shows that the dry eye group of T2DN had the mean age, median duration of DM, the ratio of females, hypertension, peripheral nerve complications, anemia, glucose, HbA1C, plasma urea, creatinine, CRP-hs, the proportion of using insulin higher than those of T2DN without dry eye, p< 0.05, 0.001. In particular, the T2DN group with dry eyes had a higher OSDI scale, and the TBUT was lower than the T2DN group without dry eyes, p< 0.001.
 |
Table 2 Comparison of Demographic and Laboratory Characteristics in Patient Diabetic Nephropathy with and without Dry Eye (n=169) |
Based on the multivariate logistic regression model in Table 3, we found that older age, female, high HbA1C, and decreased eGFR were independent factors associated with dry eye in T2DN patients, p< 0.05, 0.001.
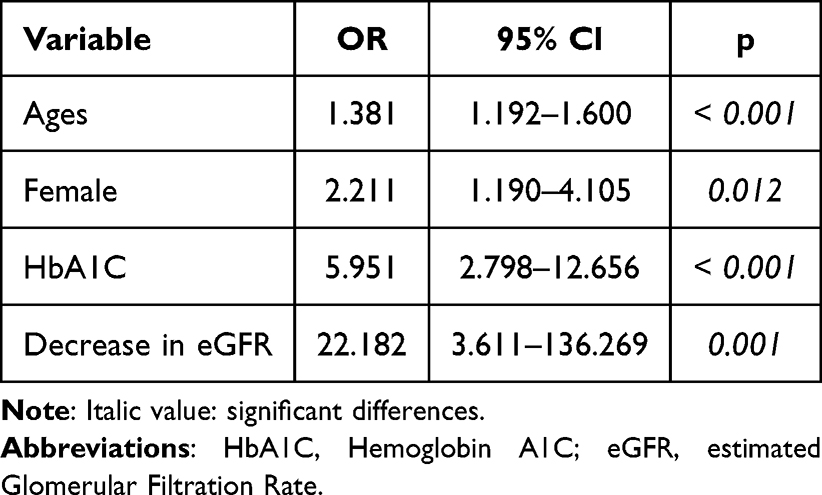 |
Table 3 Multivariate Logistic Regression Analysis of Some Clinical Variables Related to Dry Eye in Diabetic Nephropathy Patients (n=169) |
Discussion
Prevalence of Dry Eye in Patients with Type 2 Diabetic Nephropathy
The prevalence of dry eye in T2DN patients was 55.6% (94/169 patients), higher than that of T2DM (37.3% = 63/169 patients), p< 0.001. Many authors worldwide have published the prevalence of dry eyes in T2DM. In 2013, Najafi et al reported a dry eye prevalence of 27.7% in a study performed on 243 patients with type 2 diabetes mellitus.17 In 2018, in a study on 1360 T2DM, Zho et al found 238 patients, accounting for 17.5% of dry eyes.18 In 2021, De Freitas et al studied 120 diabetic patients, including 24.1% type 1 DM and 75.8% type 2 DM patients. The study’s dry eye prevalence was 38.3%.9 Recently, in 2023, the study of Mansuri et al on 105 patients with type 2 DM found the dry eye prevalence was 43.81% (92/210 eyes).10 Thus, the prevalence of dry eyes in our T2DM patients is similar to that of previous published studies.
The results of our study show that the prevalence of dry eyes in the group of T2DN patients is higher than that of the T2DM group without kidney complications (Table 1). There are no separate studies on dry eye in T2DN patients. However, our results are consistent with the cohort study by Pan et al,19 which suggested that dry eye increased with a decline in renal function in T2DM patients. In patients with type 2 diabetes, dry eye is associated with several mechanisms, including (1) lacrimal unit dysfunction, (2) abnormal enzyme metabolism and reduced mucus secretion leading to abnormal tear dynamics, (3) lacrimal gland dysfunction due to diabetic neuropathy, and (4) tear film dysfunction.7 Diabetes-related dry eye is the result of risk factors, including chronic hyperglycemia, diabetic periphery neuropathy, decreased insulin levels, microvasculopathy, and systemic hyperosmotic disturbances.7,20,21 For T2DN patients, dry eye will increase in incidence and severity due to the effects of chronic kidney disease, especially the decrease in glomerular filtration rate. Recently, dry eye has been considered a disease whose pathogenesis involves metabolic, immunological, and oxidative stress disorders.22 Dry eye is a common problem associated with inflammation, uremia, and arterial calcification due to impaired calcium-phosphorus metabolism, a common disorder in chronic kidney disease patients, including maintenance hemodialysis.23,24
The Relationship Between Dry Eyes and Some Characteristics of Patients with Type 2 Diabetic Nephropathy
To consider factors associated with dry eyes in T2DN patients, we compared the clinical and subclinical indicators between 2 groups of patients with and without dry eyes. The results showed that old age, female gender, increased HbA1C, and decreased GFR were independent factors closely related to dry eye, p<0.001 (Tables 2 and 3). Advanced age is a factor associated with dry eyes, which many authors have published in the results of previous studies on both T2DM and renal failure patients.7–9,24 Aging is associated with several risk factors for dry eye, including changes in ocular surface physiology and neurosensory abnormalities.25 An association between dry eye and HbA1C has been reported in several studies in T2DM patients.7,17,19 High HbA1C level represents chronic hyperglycemia, which increases tear glucose levels, leading to hyperosmolarity, a risk factor for dry eye.26 In addition, hyperglycemia initiates an inflammatory cascade that generates innate and adaptive immune responses in the lacrimal function unit.7 Besides the characteristics of T2DM patients, the features of renal complications also increase the prevalence and severity of dry eye. Reduced glomerular filtration rate in patients with T2DN causes accumulation of urea toxins, from which organ disorders appear, including hypertension, anemia, chronic inflammation, calcium-phosphorus disorders, and immune response. These are risk factors for increased microvascular damage and secretion disorders, which damage the ocular surface and cause dry eyes.14,23,24
Although the research goal has been achieved, our study still has some limitations because it has not fully analyzed the relationship between dry eyes and related factors in T2DN patients.
Conclusion
Dry eye was common in T2DN patients, accounting for 55.6% (94/169 patients). Factors associated with dry eye include advanced age, prolonged disease duration, anemia, decreased plasma albumin, increased HbA1C, increased CRP-hs level, and decreased GFR, in which advanced age, increased HbA1C, and decreased GFR were independently associated factors.
Human and Animal Rights
Animals did not participate in this research. All human research procedures followed the ethical standards of the committee responsible for human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Ethics Approval and Consent to Participate
This study was approved by the Ethical Committee of Nghe An Eye Hospital (No.0789/QĐ-BVMNA).
Consent for Publication
Informed consent was obtained from all the participants.
Acknowledgments
In this study, we were strongly supported by our local hospital and university in completing our research.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Lemp MA, Foulks GN. The definition and classification of dry eye disease: report of the Definition and Classification Subcommittee of the International Dry Eye Workshop (2007). Ocul Surf. 2007;5(2):75–92. doi:10.1016/S1542-0124(12)70081-2
2. Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II Epidemiology Report. Ocul Surf. 2017;15(3):334–365. doi:10.1016/j.jtos.2017.05.003
3. Tananuvat N, Tansanguan S, Wongpakaran N, et al. Reliability, validity, and responsiveness of the Thai version of the Dry Eye-Related Quality-of-Life Score questionnaire. PLoS One. 2022;17(7):e0271228. eCollection 2022. doi:10.1371/journal.pone.0271228
4. Recchioni A, Aiyegbusi OL, Cruz-Rivera S, et al. A systematic review assessing the quality of patient reported outcomes measures in dry eye diseases. PLoS One. 2021;16(8):e0253857. doi:10.1371/journal.pone.0253857
5. Basilious A, Xu CY, Malvankar-Mehta MS. Dry eye disease and psychiatric disorders: a systematic review and meta-analysis. Eur J Ophthalmol. 2022;32(4):1872–1889. doi:10.1177/11206721211060963
6. International Diabetes Federation. IDF Diabetes Atlas. 10th ed. Brussels, Belgium: International Diabetes Federation; 2021. Available from: https://www.diabetesatlas.org. Accessed April 23, 2024.
7. Zhang X, Zhao L, Deng S, et al. Dry eye syndrome in patients with diabetes mellitus: prevalence, etiology, and clinical characteristics. J Ophthalmol. 2016;2016:8201053. doi:10.1155/2016/8201053
8. Ozdemir M, Buyukbese MA, Cetinkaya A, et al. Risk factors for ocular surface disorders in patients with diabetes mellitus. Diabet Res Clin Pract. 2003;59(3):195–199. doi:10.1016/s0168-8227(02)00244-9
9. De Freitas GR, Ferraz GAM, Gehlen M, et al. Dry eyes in patients with diabetes mellitus. Prim Care Diabetes. 2021;15(1):184–186. doi:10.1016/j.pcd.2020.01.011
10. Mansuri F, Bhole PK, Parmar D. Study of dry eye disease in type 2 diabetes mellitus and its association with diabetic retinopathy in Western India. Indian J Ophthalmol. 2023;71(4):1463–1467. doi:10.4103/IJO.IJO_2770_22
11. Wei J, Wei Q, Li T, et al. Acupuncture for patients with type 2 diabetes mellitus with dry eye: protocol for a systematic review and meta-analysis. BMJ Open. 2022;12(6):e057289. doi:10.1136/bmjopen-2021-057289
12. Li B, Sheng M, Li J, et al. Tear proteomic analysis of Sjögren syndrome patients with dry eye syndrome by two-dimensional-nano-liquid chromatography coupled with tandem mass spectrometry. Sci Rep. 2014;4(1):5772. doi:10.1038/srep05772
13. Rahman EZ, Lam PK, Chu C-K, et al. Corneal sensitivity in tear dysfunction and its correlation with clinical parameters and blink rate. Am J Ophthalmol. 2015;160(5):858–866. doi:10.1016/j.ajo.2015.08.005
14. Jonas JB, Wang YX, Wei WB, et al. Chronic kidney disease and eye diseases: the Beijing Eye Study. Ophthalmology. 2017;124(10):1566–1569. doi:10.1016/j.ophtha.2017.04.024
15. Prigol AM, Tenório MB, Matschinske R, et al. Translation and validation of ocular surface disease index to Portuguese. Arq Bras Oftalmol. 2012;75(1):24–28. doi:10.1590/s0004-27492012000100005
16. Bron AJ, Abelson MB, Ousler G, et al. Methodologies to diagnose and monitor dry eye disease: report of the diagnostic methodology subcommittee of the International Dry Eye WorkShop. Ocul Surf. 2007;5(2):108–152. doi:10.1016/S1542-0124(12)70083-6
17. Najafi L, Malek M, Valojerdi AE, et al. Dry eye and its correlation to diabetes microvascular complications in people with type 2 diabetes mellitus. J Diabetes Complications. 2013;27(5):459–462. doi:10.1016/j.jdiacomp.2013.04.006
18. Zou X, Lu L, Xu Y, et al. Prevalence and clinical characteristics of dry eye disease in community-based type 2 diabetic patients: the Beixinjing eye study. BMC Ophthalmol. 2018;18(1):117. doi:10.1186/s12886-018-0781-7
19. Pan LY, Kuo YK, Chen TH, et al. Dry eye disease in patients with type II diabetes mellitus: a retrospective, population-based cohort study in Taiwan. Front Med. 2022;9:980714. eCollection 2022. doi:10.3389/fmed.2022.980714
20. Zhmud T, Malachkova N, Rejdak R, et al. Dry eye disease severity and impact on quality of life in type II diabetes mellitus. Front Med. 2023;10:1103400. eCollection. doi:10.3389/fmed.2023.1103400
21. Zhmud T, Drozhzhyna G, Malachkova N. Evaluation and comparison of subjective and objective anterior ocular surface damage in patients with type 2 diabetes mellitus and dry eye disease. Graefes Arch Clin Exp Ophthalmol. 2023;261(2):447–452. doi:10.1007/s00417-022-05806-3
22. Heidari M, Noorizadeh F, Wu K, et al. Dry eye disease: emerging approaches to disease analysis and therapy. J Clin Med. 2019;8(9):1439. doi:10.3390/jcm8091439
23. Tokuyama T, Ikeda T, Sato K, et al. Conjunctival and corneal calcification and bone metabolism in hemodialysis patients. Am J Kidney Dis. 2002;39(2):291–296. doi:10.1053/ajkd.2002.30548
24. Le Trung N, Quoc Toan P, Thang LV, et al. The relationship between dry eye in adults with indications for kidney transplantation and influence factors. Clin Ophthalmol. 2021;15:4327–4332. eCollection 2021. doi:10.2147/OPTH.S335989
25. Barabino S. Is dry eye disease the same in young and old patients? A narrative review of the literature. BMC Ophthalmol. 2022;22(1):85. doi:10.1186/s12886-022-02269-2
26. Liu H, Sheng M, Liu Y, et al. Expression of SIRT1 and oxidative stress in diabetic dry eye. Int J Clin Exp Pathol. 2015;8(6):7644–7653. eCollection 2015.
Entertainment news
Lessons learned: Strategies for future pandemic response based on mpox experience – News-Medical.Net

Targeted support for marginalized communities, strong public messaging and a properly coordinated Government approach led by Ministers are amongst the recommendations contained in a new evidence-based article examining how the UK should respond to future pandemics.
Published by The University of Manchester’s policy engagement unit, Policy@Manchester, Dr Maurice Nagington, Dr Jeremy Williams and Dr Jaime Garcia-Iglesias set out key findings from their research on how the country tackled the 2022 outbreak of mpox, formerly known as monkeypox.
Their conclusions were informed by interviews and focus groups with stakeholders including affected communities and healthcare workers.
The academics found “shortcomings in national leadership, stark local and regional inequalities in relation to vaccine access, and inadequate communication infrastructures.”
They offer advice to policymakers and public health officials in four key areas for addressing future infectious disease outbreaks, beginning with reflections on how mpox disproportionately affected marginalized communities.
“People from BAME backgrounds appeared to have lower levels of accessing the vaccine, while those from lower-income populations faced additional barriers to engaging with health and care services,” they observe. “Some individuals also faced challenges in self-isolation such as financial or emotional difficulties.”
They advise: “Public health teams need to be empowered to give additional support (such as financial) where necessary so people can self-isolate.”
The team argue that the needs of marginalized individuals merit equally important consideration when developing effective communications strategies, a second area examined in their article.
“We note social media emerged as a powerful tool in the response to the mpox outbreak, facilitating rapid dissemination of information, promoting awareness, and helping collaboration of a wide range of actors involved in the mpox response,” Nagington, Williams and Garcia-Iglesias write. “The reliance on social media also poses challenges, particularly in terms of equitable access to information.”
In their view, “additional forms of communication that can reach individuals who are marginalized should also be simultaneously developed during outbreaks.” They add: “Community organizations play an important role in developing and distributing information that is suitable and impactful.”
Addressing a third area where they believe action is needed, the academics call for Government agencies – primarily the Department for Health and Social Care – to produce guidance for local public health teams to follow, backed by additional financial support.
They recommend: “Governments should provide Ministerial level co-ordination to ensure all relevant professionals, policymakers and community representatives work together to proactively address any emerging inequalities in the immediate outbreak and plan for future outbreaks.”
And, with knowledge gained from their research of the “pivotal role” played by sexual health services during the mpox outbreak, Nagington, Williams and Garcia-Iglesias call for policymakers and legislators to “secure adequate funding and support for sexual health services to enhance their capacity to address the demands of outbreaks.”
‘Did the UK fail in its management of mpox? Lessons for future pandemics’ by Dr Maurice Nagington, Dr Jeremy Williams and Dr Jaime Garcia-Iglesias can be read free of charge on the Policy@Manchester website.
Entertainment news
Sarcopenic Obesity Exercise Intervention Program | CIA – Dove Medical Press

Introduction
Sarcopenic Obesity (SO) is a condition characterized by the coexistence of excessive obesity and loss of muscle mass or muscle function, and is prevalent in the elderly population.1 According to the Health and Nutrition Examination Survey, the prevalence of SO is 12.6% in males and 33.5% in females,2 and with the rapid growth of the global elderly population, it is estimated that 100–200 million people will be affected by SO by the year 2051.3 SO reduces the quality of life of the patients, and induces the risk of fall, fracture, disability, or increased mortality.4 Currently, there is no cure for SO, and its main treatments include exercise intervention, nutritional intervention, bariatric surgery and drug intervention; among them, the effect of exercise intervention to improve sarcopenic obesity is more certain.5,6 Exercise may delay the onset and progression of SO by modulating protein metabolism, inflammatory responses, mitochondrial function, and muscle factors.7 Aerobic exercise reduces adipose tissue and helps treat obesity by increasing energy expenditure and improving insulin sensitivity.8,9 Resistance exercise promotes the increase of skeletal muscle mass, muscle strength and fat tissue reduction in the elderly.10 However, there is no clear exercise guideline for patients with sarcopenic obesity, and the existing research focuses on the evaluation of the effect of exercise intervention in patients with sarcopenic obesity,11,12 which has not yet formed a systematic and targeted exercise practice program. For this reason, we aimed to systematically search and analyze the literature, collating, conducting, and summarizing previous research results, and constructing an exercise intervention program for patients with sarcopenic obesity. On the basis of an evidence-based approach, we hope it can provide a useful reference for the relevant personnel to develop the exercise program for patients with sarcopenic obesity.
Materials and Methods
Establishment of Research Group
The team consisted of one nursing faculty member (Ph.D., associate professor), one rehabilitation medicine faculty member (Ph.D., lecturer), one endocrinologist (M.S., attending physician), and two nursing graduate students (M.S. in progress). The graduate nursing students were responsible for literature search, screening, and quality assessment, the rehabilitation medicine faculty member and the endocrinologist were responsible for extracting information and constructing the first draft of the protocol, and the nursing faculty member was responsible for contacting the correspondence experts. The members of the team worked together to organize and analyze the results of the correspondence.
Construction of the First Draft of the Program
Theoretical Foundation
The COM-B theoretical model proposed by Michie et al13 scholars elaborate that human behavior change is influenced by ability, opportunity and motivation. Ability refers to the physical and mental abilities required to perform a specific behavior; opportunity refers to the conditions for performing a behavior in a specific environment, including physical and social opportunities; and motivation refers to the desire or intrinsic drive to perform a behavior, including reflective and spontaneous motivation.14 In developing the exercise intervention program, the COM-B theoretical model was used as a guide, and ability, motivation, opportunity, and behavior were used as first-level indicators. Physical health status and environmental influences were used as ability factors, disease knowledge, health education, and social support as opportunity factors, and self-intentions, etc., as motivational factors to promote the generation and maintenance of patients’ exercise behaviors.
Literature Search
In accordance with the “6S” (Systems, Summaries, Synopses of synthese, Syntheses, Synopses of Studies, Studies)evidence resource pyramid model,15 the literature related to exercise interventions for patients with sarcopenic obesity was systematically searched in the International Guidelines Collaboration, the website of the Association of Registered Nurses of Ontario (ARNO) in Canada, the websites of the guideline networks and professional associations such as Medline, the database of the Centre for Evidence-Based Health Care of the Joanna Briggs Institute (JBI) in Australia, the Cochrane Library, OVID, Embase, PubMed, China Knowledge Network (CKN), Vip, Wanfang and other databases. Using a combination of Mesh words and free words, “sarcopenic obesity/obese sarcopenic/obese sarcopenic/obese sarcopenic/obese sarcopenic” and “Physical activity/exercise” were the Chinese search terms. “Sarcopenic obesity/sarcopenic obese/obese sarcopenic/sarcopenia obesity/obese sarcopenia” “exercise/exercises/physical Activity/physical Exercise/acute Exercise/isometric Exercise/aerobic Exercise/exercise Training/resistance exercise” were the English search terms. Meanwhile, “sarcopenia/muscle sarcopenia/skeletal muscle loss/muscle wasting syndrome”, “exercise intervention/exercise/training/resistance training/exercise/aerobic exercise/physical activity/exercise” were used as the search terms in Chinese, “sarcopenia” “exercise/exercises/physical Activity/physical Exercise/acute Exercise/ isometric Exercise/aerobic Exercise/exercise Training/resistance exercise” as English search terms, search guidelines, expert consensus and evidence summaries. The search terms are “obesity” in Chinese, “obesity” in English, search guidelines and expert consensus. The search period is from January 2018 to June 7, 2023. Using PubMed as an example, the search form is (“sarcopenic obesity” or “sarcopenic obesity” or “obese sarcopenic” or “sarcopenic obesity” or “obese sarcopenic”) and (“exercise” or “sport” or “physical activity” or “physical activity” or “acute exercise” or “isokinetic exercise” or “aerobic exercise” or “athletic training” or “resistance exercise”).
Literature Inclusion and Exclusion Criteria
Inclusion Criteria: ① The study subjects were patients with sarcopenic obesity; ② The content was exercise intervention or exercise management for patients with sarcopenic obesity; ③ Publicly available guidelines, evidence summaries, expert consensus, systematic evaluations and Meta-analyses; ④ Inclusion of the latest version of the guidelines; ⑤ The language was Chinese or English.
Exclusion criteria: ① Incomplete information or inaccessible full-text literature; ② Repeatedly published literature; ③ Literature with low quality evaluation.
Literature Screening and Quality Assessment
The methodological quality of all included literature was independently evaluated by 2 researchers who have systematically studied evidence-based nursing, and a third evidence-based nursing researcher arbitrated when there was a disagreement in the evaluation. Guidelines were evaluated for methodological quality using the Appraisal of Guidelines for Research and Evaluation Instrument for Clinical Practice (AGREE II),16 and expert consensus was evaluated for methodological quality using the JBI Center for Evidence-Based Health Care Expert Consensus Evaluation Criteria,14 retrospective evidence summarization of original studies, quality evaluation of original literature using quality evaluation tools proposed by the JBI Centre for Evidence-Based Health Care in Australia for different types of studies, and systematic evaluation and Meta-analysis using the Assessment of Multiple Systematic Reviews 2 (AMSTAR2) for methodological quality assessment.17
Development of the First Draft of the Program
After completing the quality assessment, two researchers trained in evidence-based nursing independently extracted and synthesized evidence from the included literature to form a first draft of the exercise intervention protocol. In case of disagreement during the extraction process, a third evidence-based nursing researcher arbitrated.
Delphi Method
Preparation of the Questionnaire
According to the first draft of the program and the purpose of the Delphi method research group prepared the questionnaire, which consists of three parts: ① Questionnaire description mainly introduces the background of the study, the purpose of the study and instructions for filling out the form. ② The body of the questionnaire refers to the experts evaluation of the exercise intervention program for patients with sarcopenic obesity, the importance of each entry is rated from 1 to 5, with 1 representing very unimportant and 5 representing very important, and an opinion column is set up after each entry for experts to provide suggestions. ③ Questionnaire on basic information of experts.
Expert Selection Criteria
① Endocrinologists, rehabilitation doctors, sports rehabilitation therapists, geriatric specialist nurses, etc.; ② More than 10 years of work experience in the related work field; ③ With undergraduate education or above, intermediate or above titles; ④ Voluntary participation in this study, able to provide timely feedback results, and to provide valuable suggestions for the content of the program.18
Implementation of Delphi Method
Fifteen experts were selected for questionnaire correspondence, and the questionnaires were distributed by e-mail and returned within 14 days after distribution. According to the results of the first round of expert consultation, the mean value of the importance score >4 and the Coefficient of Variation (CV) <0.25 were taken as the screening criteria, and each specific opinion of the experts was added, modified or deleted accordingly to form the second round of the questionnaire, and the consultation was terminated when the experts’ opinions converged.
Statistical Methods
SPSS 26.0 software was used for data analysis. Measurement data were described by ( ), and count data were statistically described by frequency and percentage. Expert positivity was expressed by the effective recovery rate of the questionnaire and the rate of expert opinions presented. The degree of expert authority was expressed by the coefficient of expert authority (Cr), which was determined by the degree of familiarity (Cs) and the basis of judgment (Ca) of the experts. The degree of expert opinion coordination was expressed by the coefficient of variation (CV) and Kendall’s coordination coefficient (Kendall’s W).
), and count data were statistically described by frequency and percentage. Expert positivity was expressed by the effective recovery rate of the questionnaire and the rate of expert opinions presented. The degree of expert authority was expressed by the coefficient of expert authority (Cr), which was determined by the degree of familiarity (Cs) and the basis of judgment (Ca) of the experts. The degree of expert opinion coordination was expressed by the coefficient of variation (CV) and Kendall’s coordination coefficient (Kendall’s W).
Results
First Draft of the Program
A total of 1306 articles were identified through the initial search. After deleting duplicates, further screening and quality evaluation using Endnote20 software, 12 articles were finally included, including 2 guidelines,19,20 2 expert consensus articles,1,21 1 evidence summary article,22 5 systematic evaluations,7,11,23–25 and 2 Meta-analyses.26,27 Through literature reading and evidence extraction, the first draft of the exercise intervention program contains 4 primary indicators, 12 secondary indicators, and 29 tertiary indicators. The quality evaluation of the included literature is showed in Supplementary Tables 1–3.
Results of Delphi Method
General Information of Experts
Fifteen experts in related fields were finally included in this study, and all experts completed 2 rounds of correspondence. Their ages ranged from 38 to 53 (44.53±4.90) years old; their working years ranged from 11 to 35 (20.67±7.61) years; they had 9 PhDs, 2 master’s degrees, and 4 bachelors’ degrees; they had 4 full-senior titles, 7 vice-senior titles, and 4 intermediate titles; among them, there were 4 experts in clinical medicine, 4 experts in rehabilitation medicine, 2 experts in medical technology, and 5 experts in clinical nursing and geriatric nursing.
The Degree of Motivation and Authority of Experts
Fifteen questionnaires were issued for the 2 rounds of Delphi method, and 15 valid questionnaires were recovered, with a 100% effective recovery rate of the questionnaires. The rate of expert opinions presented was 73% and 60% respectively. The Ca, Cs, and Cr of the experts in the 1st round were 0.97, 0.7, and 0.83, respectively. The Cs, Ca, and Cr of the experts in the 2nd round were 0.97, 0.66, and 0.82, respectively.
Degree of Harmonization of Expert Opinions
The coefficient of variation of the 1st round of Delphi method was 0.00–0.27, and the importance score was (4.13±1.13)~(5±0); the coefficient of variation of the 2nd round was 0.00–0.20, and the importance score was (4.53±0.64)~(5±0); the coefficients of Kendall’s harmonization were 0.102, and 0.115, respectively, and the differences were statistically significant (p<0.05).
Summary of Expert Opinions and Modifications
The panel made the following adjustments to the program indicators based on expert opinions, screening criteria and statistical results:
The first round of expert consultation: ① Deletion of 2 entries: Deletion of 2 Level 3 indicators with coefficient of variation > 0.25 “1.1.2 Recording aerobic exercise and resistance exercise teaching videos according to Fitness Qigong – Baduanjin” and “Elastic band strength exercise program” recommended by the State General Administration of Sport. “Record aerobic exercise and resistance exercise teaching videos” and “4.5.5 Make exercise score cards, record the number of lectures attended and exercises participated, and set up corresponding reward mechanisms”.② Modification of 14 entries: the modifications are mainly describing the specialists who conduct the assessment, evaluating the patient’s fitness level and refining the contraindications; adding a rehabilitation therapist to conduct the exercise instruction and reorganizing this entry as a social opportunity; combining entries 1.2.1 and 1.2.2 and focusing on improving the patient’s psychological competence; adjusting the entries’ serial numbers 2.1.2 and 2.1.3; continuing to follow up on the reasons affecting the patient’s exercise and concerns; increasing social opportunities such as environmental and fitness resources; expanding social support beyond family and friends; adding rehabilitation physicians to the study team; increasing forms of aerobic exercise; adjusting individualized choices of elastic bands; increasing core muscle training; adjusting the duration of exercise; combining entries 4.5.1 and 4.5.3; and adding observations of exercise injuries.
The 2nd round of Delphi method: ① Modification of 7 entries: the modifications were to add objective indicators of relative contraindications; to interchange level 2 indicators 2.2.1 and 2.2.2; to increase the number of training staff; to merge entries 4.1.4 and 4.1.5; to adjust the descriptions of the duration of the exercise; to supplement the descriptions of the intensity of the exercise; and to modify the descriptions of the adjustment of the intensity of the exercise.
The final result was an exercise intervention program for patients with sarcopenic obesity with 4 indicators at level 1, 12 indicators at level 2, and 28 indicators at level 3, as shown in Table 1, and a thumbnail sketch of an exercise intervention programs is showed in Supplementary Figure 1.
 |
Table 1 Exercise Intervention Program for Patients with Sarcopenic Obesity |
Discussion
The Exercise Intervention Program for Patients with Sarcopenic Obesity is Scientific and Feasible
Based on the COM-B theoretical model and evidence-based methodology, this study searched the literature layer by layer according to the “6S” evidence resource pyramid model, and after repeated selection and quality evaluation by two people, the high quality literature was included, the evidence was extracted and summarized to form the first draft of the exercise intervention program, and after two rounds of experts’ correspondence, the final program was determined, and the methodology of the intervention program was scientifically sound.
The 15 experts who participated in the correspondence were from the fields of clinical medicine, rehabilitation medicine, medical technology, and nursing, all of whom had solid theoretical foundations and rich clinical practice experience. The effective recovery rate of the questionnaires for the 2 rounds of Delphi method was 100%, and the rate of expert opinions presented was 73% and 60%, respectively, indicating that the experts in the two rounds of consultation had a high degree of motivation. In general, an expert’s authority coefficient higher than 0.7 is considered acceptable, and ≥0.8 indicates a high degree of expert authority.28 In this paper, the expert authority coefficients are 0.83 and 0.82 respectively, indicating that the correspondence results are authoritative and reliable. The smaller the coefficient of variation, the higher the degree of harmonization of experts,29 the coefficient of variation in this paper is 0.00~0.27 and 0.00~0.20, respectively, indicating that the experts’ opinions are more consistent. Kendall’s harmony coefficient ranges from 0 to 1, the closer to 1 indicates that the better the degree of coordination,30 the Kendall’s harmony coefficient of correspondence in this paper were 0.102, 0.115 (P < 0.05), although not close to 1, but the value of the second round increased, indicating that the experts have achieved a higher degree of consensus, the degree of coordination of the correspondence is good, and the contents of the program constructed are scientific and feasible.
The Constructed Exercise Intervention Program for Patients with Sarcopenic Obesity is Operable and Applicable
Based on the COM-B theoretical model, this study considers the three dimensions of ability, motivation, and opportunity comprehensively to ensure that patients receive the best support and guidance in exercise. ① Ability: the patients’ potential to perform exercise was assessed from both physical and mental ability aspects. In terms of physical ability, the rehabilitation physician assesses whether the patient has absolute and relative contraindications to exercise. The psychological ability of patients is improved through group sharing and exchange sessions. ② Motivation: Through health lectures, patients are taught the basic knowledge of sarcopenic obesity disease and the role and significance of exercise interventions to improve their spontaneous motivation and to improve their reflective motivation by continuously understanding their willingness to exercise and the factors influencing them during the exercise process. ③ Opportunity: provide patients with physical opportunities through the choice of personalized exercise programs, and social opportunities through the support of family and friends and the surrounding environment. ④ Behavior: Under the joint action of ability, motivation and opportunity, it promotes the emergence of patients’ exercise behavior. This plan puts forward multi-mode exercise therapy. Aerobic exercise can not only oxidize sugar in the body, burn fat in the body, enhance and improve heart and lung health, but also prevent osteoporosis. Among them, walking, aerobics and cycling are the main aerobic exercise methods.31
Resistance exercise is training for different muscle groups, which can enhance muscle quality and strength by stimulating muscle protein synthesis. Elastic belt, dumbbells, barbells and weighted sandbags are often used for resistance exercise.32,33 Resistance combined with aerobic exercise is better than single exercise in improving muscle strength, which is consistent with the research results of Hsu et al.26 National and international standards and expert consensus21 state that exercise intensity should be moderate to high intensity. In summing up the characteristics of resistance training programs for patients with sarcopenia obesity, Silva pointed out that more than half of the studies chose the exercise intensity range of 40% to 85% of 1 Repetition Maximum (1 Repetition Maximum, 1RM).34 However, in the actual operating environment, it is challenging to achieve accurate measurement and evaluation of 1RM. Because it is difficult to determine the difference of 1RM and each study often uses different measurement tools. Therefore, this protocol recommends that the resistance exercise intensity on Borg’s conscious exercise table should be 12 to 14 points, and the aerobic exercise intensity should be 50% to 80% of the limit heart rate. This protocol suggests 40–50 minutes of exercise each time, and the intervention frequency is 2–3 times/week for 12 weeks, which is consistent with the suggestion of the British physical activity guide, that is, all elderly people should do 150 minutes of moderate intensity exercise or 75 minutes of intense intensity exercise twice a week. Eglseer et al believe that two or three times a week of exercise training can effectively reduce the percentage of body fat and improve muscle mass, muscle strength and gait speed.24 This study states that patients’ vital signs and the presence of adverse events should be monitored during exercise, providing assurance of patient exercise safety.21 It is also recommended to assess the changes in patients’ fitness level and quality of life, etc. at the end of the intervention to evaluate the effectiveness of exercise intervention in patients with sarcopenic obesity.
Limitations and Outlook
This work has two limitations. First, based on the feasibility and applicability of the exercise program, we currently use elastic belt to carry out resistance exercise. Although other types of resistance exercise, such as dumbbells, barbells and tensioners, have a significant impact on the improvement of muscle quality and strength, they require the elderly with SO to have a higher degree of balance and coordination, and we will study this issue in the future. Second, based on the lack of exercise intervention guidelines and expert consensus for sarcopenia obesity, this work systematically analyzes the guidelines and evidence related to sarcopenia and obesity, and constructs a new intervention plan. However, the effectiveness and feasibility of the intervention scheme constructed in this work need to be verified by clinical trials in the future. Therefore, when applying the intervention plan constructed in this work, it is suggested that it should be combined with rehabilitation or exercise intervention, and a professional team should formulate an individualized and feasible exercise intervention plan according to the patient’s physical condition and living environment, so as to improve the quality of life of patients.
Conclusion
Based on the COM-B theoretical model and evidence-based principles, this study constructed an exercise intervention program for patients with sarcopenic obesity (including 4 aspects and 28 entries) by adopting the methods of evidence-based nursing and Delphi method, which provides a new path for exercise therapy for patients with sarcopenic obesity and has clinical value.
Ethical/Copyright Corrections
This manuscript is an analysis report of literature and expert opinions, and does not involve personal privacy or sensitive information. Hence, it does not require the approval of ethics committees.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Donini LM, Busetto L, Bischoff SC, et al. Definition and diagnostic criteria for sarcopenic obesity: ESPEN and EASO consensus statement. Obesity Facts. 2022;15(3):321–335. doi:10.1159/000521241
2. Batsis JA, Mackenzie TA, Emeny RT, Lopez-Jimenez F, Bartels SJ. Low lean mass with and without obesity, and mortality: results from the 1999–2004 national health and nutrition examination survey. J Gerontol a Biol Sci Med Sci. 2017;72(10):1445–1451. doi:10.1093/gerona/glx002
3. Lee DC, Shook RP, Drenowatz C, Blair SN. Physical activity and sarcopenic obesity: definition, assessment, prevalence and mechanism. Future Sci OA. 2016;2(3):Fso127. doi:10.4155/fsoa-2016-0028
4. Someya Y, Tamura Y, Kaga H, et al. Sarcopenic obesity is associated with cognitive impairment in community-dwelling older adults: the Bunkyo health study. Clin Nutr. 2022;41(5):1046–1051. doi:10.1016/j.clnu.2022.03.017
5. Qin J, Wang M, Sun L, et al. Current status of non-pharmacologic interventions for sarcopenic obesity in the elderly. Evid Bas Nurs. 2023;9(11):1966–1969.
6. Gortan Cappellari G, Brasacchio C, Laudisio D, et al. Sarcopenic obesity: what about in the cancer setting? Nutrition. 2022;98:111624. doi:10.1016/j.nut.2022.111624
7. Ghiotto L, Muollo V, Tatangelo T, Schena F, Rossi AP. Exercise and physical performance in older adults with sarcopenic obesity: a systematic review. Front Endocrinol. 2022;13:913953. doi:10.3389/fendo.2022.913953
8. Villareal DT, Aguirre L, Gurney AB, et al. Aerobic or resistance exercise, or both, in dieting obese older adults. N Engl J Med. 2017;376(20):1943–1955. doi:10.1056/NEJMoa1616338
9. Al-Mhanna SB, Rocha-Rodriguesc S, Mohamed M, et al. Effects of combined aerobic exercise and diet on cardiometabolic health in patients with obesity and type 2 diabetes: a systematic review and meta-analysis. BMC Sports Sci Med Rehabil. 2023;15(1):165. doi:10.1186/s13102-023-00766-5
10. Fragala MS, Cadore EL, Dorgo S, et al. Resistance training for older adults: position statement from the national strength and conditioning association. J Strength Cond Res. 2019;33(8):2019–2052. doi:10.1519/jsc.0000000000003230
11. Poggiogalle E, Parrinello E, Barazzoni R, Busetto L, Donini LM. Therapeutic strategies for sarcopenic obesity: a systematic review. Article. Curr Opin Clin Met Care. 2021;24(1):33–41. doi:10.1097/MCO.0000000000000714
12. Martínez-Amat A, Aibar-Almazán A, Fábrega-Cuadros R, et al. Exercise alone or combined with dietary supplements for sarcopenic obesity in community-dwelling older people: a systematic review of randomized controlled trials. Maturitas. 2018;110:92–103. doi:10.1016/j.maturitas.2018.02.005
13. Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42. doi:10.1186/1748-5908-6-42
14. Zheng J, Han R, Wang Y, et al. Summary of the best evidence for nonpharmacologic airway clearance techniques in patients with chronic respiratory disease. Chin J Nurs. 2023;58(10):1253–1260.
15. Zhang X, Zheng Q, Wang Q, et al. Summary of the best evidence for exercise management in patients with nonalcoholic fatty liver disease. Chin J Nurs. 2023;58(20):2464–2471.
16. Brouwers MC, Kho ME, Browman GP, et al. AGREE II: advancing guideline development, reporting and evaluation in health care. Cmaj. 2010;182(18):E839–42. doi:10.1503/cmaj.090449
17. Zhang F, Shen A, Zeng X, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017; 358: j4008. doi:10.1136/bmj.j4008
18. Qu J, Zhu Y, Qu B. Application of Delphi method in medical education research. Chin J Med Educ. 2019;3:227–230.
19. Dent E, Morley JE, Cruz-Jentoft AJ, et al. International clinical practice guidelines for sarcopenia (ICFSR): screening, diagnosis and management. J Nutr Health Aging. 2018;22(10):1148–1161. doi:10.1007/s12603-018-1139-9
20. Mathus-Vliegen EM. Obesity and the elderly. J Clin Gastroenterol. 2012;46(7):533–544. doi:10.1097/MCG.0b013e31825692ce
21. Cui H, Wang Z, Wu J, et al. Chinese expert consensus on prevention and control of sarcopenia in the elderly (2023). Chin J Geriatrics. 2023;2023:(02):144–153.
22. Min W, Chen Y, Lu Q, et al. Summary of the best evidence for exercise intervention in elderly patients with sarcopenia. PLA Nursing J. 2022;39(03):75–78.
23. Zhuang M, Jin M, Lu T, et al. Effects of three modes of physical activity on physical fitness and hematological parameters in older people with sarcopenic obesity: a systematic review and meta-analysis. Front Physiol. 2022;13:917525. doi:10.3389/fphys.2022.917525
24. Eglseer D, Traxler M, Schoufour JD, et al. Nutritional and exercise interventions in individuals with sarcopenic obesity around retirement age: a systematic review and meta-analysis. Nutr Rev. 2023;81(9):1077–1090. doi:10.1093/nutrit/nuad00
25. Yin Y-H, Liu JYW, Valimaki M. Effectiveness of non-pharmacological interventions on the management of sarcopenic obesity: a systematic review and meta-analysis. Exp Gerontology. 2020;135110937. doi:10.1016/j.exger.2020.110937
26. Hsu K-J, Liao C-D, Tsai M-W, Chen C-N. Effects of exercise and nutritional intervention on body composition, metabolic health, and physical performance in adults with sarcopenic obesity: a meta-analysis. Nutrients. 2019;11(9):2163. doi:10.3390/nu11092163
27. Hita-Contreras F, Bueno-Notivol J, Martínez-Amat A, Cruz-Díaz D, Hernandez AV, Pérez-López FR. Effect of exercise alone or combined with dietary supplements on anthropometric and physical performance measures in community-dwelling elderly people with sarcopenic obesity: a meta-analysis of randomized controlled trials. Maturitas. 2018;116:24–35. doi:10.1016/j.maturitas.2018.07.007
28. Yu X, Zhang C, Hong M, et al. Construction of emergency open abdominal care plan for abdominal surgery patients with hemorrhage. Chin J Nurs. 2023;58(20):2472–2480.
29. Cheng T, To H, Xiong X, et al. Construction of a multiple medication management program for elderly patients after percutaneous coronary intervention. Chin J Nurs. 2023;58(12):1476–1482.
30. Zhu H, Wang Q, Yu H, et al. Construction of a self-management program for patients with diabetic foot amputation. Chin J Nurs. 2023;58(15):1838–1844.
31. Chen HT, Chung YC, Chen YJ, Ho SY, Wu HJ. Effects of different types of exercise on body composition, muscle strength, and igf-1 in the elderly with sarcopenic obesity. J Am Geriatr Soc. 2017;65(4):827–832. doi:10.1111/jgs.14722
32. da Silva Gonçalves L, Santos Lopes da Silva L, Rodrigues Benjamim CJ, et al. The effects of different exercise training types on body composition and physical performance in older adults with sarcopenic obesity: a systematic review and meta-analysis. J Nutr Health Aging. 2023;27(11):1076–1090. doi:10.1007/s12603-023-2018-6
33. Phillips BE, Atherton PJ, Varadhan K, et al. The effects of resistance exercise training on macro- and micro-circulatory responses to feeding and skeletal muscle protein anabolism in older men. J Physiol. 2015;593(12):2721–2734. doi:10.1113/jp270343
34. da Silva LSL, Gonçalves LDS, Abdalla PP, et al. Characteristics of resistance training-based protocols in older adults with sarcopenic obesity: a scoping review of training procedure recommendations. Front Nutr. 2023;10:1179832. doi:10.3389/fnut.2023.1179832


Dry eye and some related factors in patients with T2DN | OPTH – Dove Medical Press

Lessons learned: Strategies for future pandemic response based on mpox experience – News-Medical.Net

Sarcopenic Obesity Exercise Intervention Program | CIA – Dove Medical Press
About Us

EmPawa Business Funding – Simplifying Business Financing | With Susan Sundai

Breaking news – Chronicle
-
About Us5 months ago
About Us
-
 Business5 months ago
Business5 months agoEmPawa Business Funding – Simplifying Business Financing | With Susan Sundai
-
 money markets3 weeks ago
money markets3 weeks agoBreaking news – Chronicle
-

 gospel3 weeks ago
gospel3 weeks agoAmerican gospel artistes to grace Zim – NewsDay
-
gospel3 weeks ago
American gospel artistes to grace Zim – NewsDay
-
gospel3 weeks ago
American gospel artistes to grace Zim – NewsDay
-

 travel3 weeks ago
travel3 weeks agoZimbabwe receive Emarati travel bloggers – Chronicle
-

 soccer2 weeks ago
soccer2 weeks agoEx-PSL stars link up at new Zim club – FarPost